

INTRODUCTION
Patients with severe spinal cord injury (SCI), including complete cervical spine injuries, are highly unstable in the acute phase and require hospitalization in the intensive care unit (ICU) with continuous cardiac, hemodynamic and respiratory monitoring1,2). Respiratory complications can quickly worsen within five days of injury, so active respiratory management should be initiated3). Hemodynamic instability should also be corrected quickly because recent studies recommended preventing systemic hypotension because maintaining proper spinal cord perfusion in patients with acute SCI may reduce long-term disability1,4). Additionally, SCI patients are vulnerable to hospital-acquired infections because they spend a considerable amount of time in the hospital5). Patients with traumatic spinal injuries also accompany other polytrauma injuries6), and the inability of self-hygiene due to paralysis, reflex loss, bedsores, tracheal intubation, prolonged placement of the catheter, and steroid use makes SCI patients susceptible to different infections, making the treatment of the disease more complex and challenging7).
Methylprednisolone has been noted for its potential as a therapeutic agent for SCI due to its inhibitory effect on active oxygen-induced lipid peroxidation, an essential biochemical mechanism of early SCI8). High-dose methylprednisolone has been widely used as an main medical treatment by many spine surgeons from the 1990s to the early 2000s since the National Acute Spinal Cord Injury Studies (NASCIS)9,10). However, in several randomized clinical studies afterward, it was reported that neurological improvement was insignificantly compared to the serious side effects1,8). It was suggested that the 2013 AANA/CNS guideline announced that steroid administration is no longer recommended4). Conversely, the positive effect of steroid administration is still reported sporadically, and the 2017 AOSpine guideline recommended it as a treatment option for acute SCI within eight hours of injury11).
Early decompression of the spinal cord helps improve clinical outcomes. In a meta-analysis of clinical trials, if the duration of spinal cord compression is long, studies are showing worsened results, including neurological recovery and blood circulation disorders12). However, until recently, clinical evidence is lacking, and there are no international guidelines for the timing of surgery1,13).
Since SCI leaves severe disability in patients, several studies have been conducted on the treatment of SCI. However, it is challenging to consistently control parameters in clinical studies of SCI patients due to various trauma mechanisms, degrees of cord injury, and types of spinal surgery. In the case of a prospective study, there is also an ethical problem in randomly selecting the treatment option for patients with critical cord injury rather than the best treatment considered by the attending physician.
To relatively standardize SCI patients, patients with traumatic cervical spine injuries were confined. Among them, it was assumed that patients who received ICU treatment were critically injured patients. To find the prognostic factors in patients with SCI, a retrospective study of these ICU patients was performed.
MATERIALS AND METHODS
Patient selection and data acquisition
Traumatic cervical SCI patients treated at our hospital's ICU from February 2013 to May 2019 were retrospectively reviewed. Of the 123 traumatic SCI patients, 102 patients were included, excluding patients who were transferred to the general ward within 24 h of admission to the ICU and patients without adequate clinical data six months after the injury. Demographic data, spinal surgery, timing of surgery, tracheostomy, ventilator, steroid use, diabetes, infection, and hypotension of less than 90 mean arterial pressure within a week after injury were investigated using medical records. For clinical outcome analysis, upper and lower extremity muscle strength and ASIA impairment scale were analyzed at initial, three weeks and six months after the injury.
Statistical analyses
To discover the difference between the patient groups according to the surgery or not and the effect of surgery on the prognosis of patients, the patients were divided into two groups: the patient group who underwent surgery and the patient who did not undergo surgery. The group that underwent surgery was divided into a group that operated within 36 h after injury and a group that operated after 36 h for comparative analysis.
Categorical variables were analyzed with chi-square and Fisher’s exact tests, and continuous variables were compared with Student’s t-tests and Mann–Whitney test. Multivariable logistic regression models were later made to control the potential compounding variables. Statistical calculations were performed using SPSS version 20.0 (IBM Corp., Armonk, NY, USA).
RESULTS
The patient demographics are listed in Table 1. Among the 102 patients, 76 were male (74.5%), and 26 were female (25.5%), and the average age was 57.57 years. The average total length of hospital stay was 65.04 d, and the average length of ICU stay was 13.28 d. Eighty-seven patients (85.3%) underwent spine-related surgery, and among them, 30 patients received operation within 36 h after injury. Seventy-seven (75.5%) were with the chief complaint of trauma, while nine (8.8%) of them were accompanied by skull fracture or traumatic intracranial hemorrhage. Ten patients (9.80%) required ventilator care during the ICU stay, and four patients (3.9%) required tracheostomy. Of these, 3 patients had failed extubation for more than 3 weeks, and the remaining 1 patient was an emergency tracheotomy due to a hematoma in the anterior cervical surgical site. The steroid was administered to 15 patients (14.9%) whereas sixteen patients (15.7%) had a comorbidity of diabetes mellitus. A total of 66 (64.7%) patients required consultation with the division of infectious diseases due to infectious diseases. Meanwhile, during ICU treatment, 91 (89.2%) patients had a mean arterial pressure (MAP) of less than 90.
Table 2 shows the results of comparative analysis of 102 enrolled patients divided into two groups, 87 who underwent surgery and 15 who did not. There were no differences in sex, mean age, head trauma, tracheostomy, mechanical ventilation, steroid use, diabetes, and hypotension between the groups. On the other hand, the total number of hospitalization and ICU treatment days tended to be longer in the non-surgical group but did not reach statistical significance. However, in the case of arm motor, the surgical group was significantly better at three weeks (p=0.029), but there was no difference around six months. In the case of leg motor, the surgical group exhibited significantly better results at six months (p=0.043).
The 87 patients who underwent surgery were compared by dividing the surgical timing into two groups of 36 h from injury (Table 3). Among the total surgery patients, 30 patients (34.5%) had surgery within 36 hours, and their average age was 50.7 years, which is about 10 years younger than the late surgery group. (p=0.009). Additionally, the total hospital stay and intensive care unit treatment days were longer in the early surgery group (p=0.068 and p=0.021, respectively), and steroid use was also significantly higher (p<0.001).
To analyze the factors related to the patient's prognosis, logistic regression analysis of the parameters for neurological symptoms 3 weeks and 6 months after SCI was performed (Table 4,-6). Logistic regression analysis showed that surgery within 36 hours had a significant positive correlation with improvement in leg motor after 3 weeks of SCI (Table 4), whereas steroid use showed a significant positive correlation with improvement of leg motor after 6 months. (Table 5). Although not presented, no significant parameters were observed in the regression analysis in the case of arm motor.
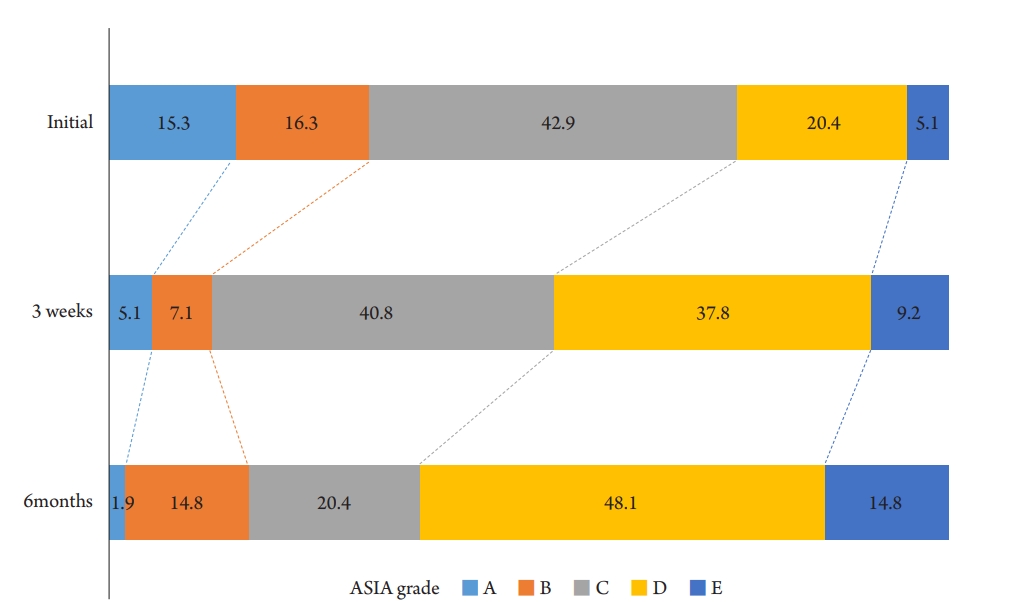
A graph comparing changes in the distribution of ASIA grade by period is indicated in Fig. 1. Initially, 42.9% of the patients were ASIA-C grade, and the most severe ASIA-A grade was 15.3%. However, after three weeks, the number of ASIA-A patients reduced to 5.1%, and the relatively mild cases of ASIA-D and E increased from 25.6%–47.0%. At six months, 1.9% of all patients were still ASIA-A grade without improvement, and patients with ASIA-D and E accounted for 62.9%, which is 2.5 times higher than the initial. A regression analysis was also conducted on the correlation between the parameters and the degree of improvement of the ASIA grade, and steroid use was significant in the degree of improvement at six months (Table 6).
In this series, 66 patients (64.7%) developed a fever during hospitalization. Of these, 63 patients were treated with antibiotics, and the remaining three were atelectasis, steroid-related, and drug fever. The sites of infection and causative microorganisms of 63 patients (22 patients had more than one type of infection) with infection are indicated in Table 7. Regarding the occurrence of infection, urinary tract infection was the most common with 35 patients (57.5%), followed by respiratory tract infection 30 (49.2%) and skin infection. The microorganism was isolated 126 times; 50 (39.7%) were gram-positive, 67 (53.2%) were gram-negative, otherwise, eight (5.6%) were fungal and one (1%) was parasitic. Between the isolated microorganism of 126, Staphylococcus aureus (S.aureus) was isolated in 18 (14.3%). MRSA was isolated in 12 (9.5%), which occupied a lot among the isolated S.aureus. Bacteria producing extended-spectrum beta-lactamase were isolated in six (4.8%).
DISCUSSION
According to the study results that hypotension has adverse effects in the early stages of traumatic SCI, it was recommended to maintain the MAP at 85-90 in the first week as a recent guideline14). In 1976, Zach et al. conducted a prospective study of 117 patients with acute SCI in the ICU, which improved neurological outcomes through early, aggressive treatment and blood pressure management15). 1991 Wolf et al. In a study of 52 patients with bilateral cervical dislocation targeting a MAP > 85-mmHg for five days, they found that the patients exhibited neurological improvement.16) In 1993, Levi et al. (1993) targeted 50 SCI patients with MAP > 90-mm Hg more aggressively than MAP > 85-mmHg, and concluded that aggressive hemodynamic support reduced mortality and morbidity17). In 1997, Vale et al. reported that 77 SCI patients treated in the ICU with a MAP > 85-mmHg target and aggressive hemodynamic support for seven days indicated clinical improvement at one year follow-up18).
In patients with SCI, Spinal ischemia, which can be exacerbated by hypotension and hypoxia, plays a vital role in the occurrence of secondary progressive injury19). Intracellular mechanism of the SCI cascade, including neurogenic shock, microhemorrhage, ischemia-reperfusion injury, apoptosis, is related to secondary SCI20). Because of the fact that ischemia, hypotension and hypoxia can exacerbate secondary SCI, blood pressure control is one of the factors that play an essential role in reducing secondary SCI. Unfortunately, in patients with ACSI, hemodynamic and autonomic instability can often be found in the early stages of injury21). In this study, MAP of less than 90-mmHg was observed in 91 of 102 patients (89.2%) during the stay in ICU. Lower MAP than the guideline may have been caused by the underestimation of the importance of maintaining MAP. Additionally, the fact that autonomic nerve instability frequently appears in patients with severe SCI probably had an impact. Currently, our center maintains a MAP of 85 or higher in patients with severe SCI, even with vasopressors.
Respiratory complications in the acute phase of spinal cord injury are the leading cause of morbidity and mortality, accounting for 80.0% of mortality in patients with cervical SCI. Moreover, the prevalence of respiratory complications is very high, reaching 36.0%–80.0%22). High mortality and morbidity in SCI patients can be explained by respiratory dysfunction due to damage of the respiratory muscles, decreased vital capacity, difficulty in sputum discharge, and decreased compliance of lung and chest wall23). And some of these patients require a ventilator, and long-term use of the ventilator will require tracheostomy23).
Tracheostomy rates in CSCI patients vary from 20.0% to 75.0%24). Although there is no clear standard for the timing of tracheostomy, some authors have argued that early tracheostomy (within 4 days) can reduce the duration of ICU hospitalization and respiratory complications, regardless of the degree of cervical spine injury25). Since we did not perform tracheostomy as it could interfere with the anterior cervical approach, the proportion of tracheostomy among all SCI patients was as low as 3.9%. We try extubation when the patient shows improvement in respiratory function, and tracheostomy is performed only for patients who have repeatedly failed extubation.
Patients with SCI are at high risk of healthcare-associated infections due to the frequent use of invasive medical devices, such as urinary and endovascular catheters. However, data on infection prevention and treatment in patients with SCI are lacking.26) Respiratory infections in patients with SCI are the most common during initial hospitalization, with a frequency of 60%. Streptococcus pneumoniae was the most common causative agent, and the prevalence of Pseudomonas was also observed to be high. Similarly, our study showed that Pseudomonas is the most prevalent cause of respiratory infection. Additionally, in patients with SCI, the typical pneumonia symptom occurrence rate is relatively low, making it challenging to detect pneumonia immediately. In our study, respiratory tract infection occurred in 30 patients (49.2%), and ten (9.8%) received ventilator treatment. Four patients (3.9%) underwent tracheostomy. So, it is crucial to ensure adequate preventive measures, such as vaccination against pneumonia26).
Urinary tract infection (UTI) is reported to develop within the first 50 d in 22% of patients with acute SCI, and is a significant cause of patient mortality and morbidity27). It is associated with urinary catheterization, and E. coli is the most common causative organism, which is the same as the results of this study. Even though the prevalence of UTI is high, the prevention method is unclear26). Considering the high prevalence of UTI in patients with SCI, periodic urine culture is suggested even when asymptomatic.
Bedsores also frequently act as a cause of infection in SCI patients. As a result of the bacteriological study of infected bedsores conducted by Heymet et al., the most frequently identified bacteria were Enterobacteriaceae group, accounting for 29%, and Staphylococcus spp. It was followed by 28% (mostly S. aureus)28). In our series, although relatively few compared to the previous literature, bedsore-related infections occurred in 14.8% of patients, mostly due to Staphylococcus aureus. Rapid identification and treatment of severe infections within the first 24 h after onset with appropriate antibiotics is associated with better outcomes. However, nearly 40% of SCI patients do not get adequate initial empirical antibiotic therapy26). In order to quickly identify an infection, we immediately and simultaneously perform blood, sputum, and urine cultures when a fever occurs. And before the causative organism is identified, empirical antibiotics are administered early through consultation with the Division of Infectious Diseases.
The American Spinal Injury Association (ASIA) Impairment Scale is commonly used to classify the neurological severity of SCI29), and is also being used because it is essential to view the prognosis of patients with SCI accurately30). In 2009, Martina R et al. conducted a cohort study in which SCI patients were classified using ASIA grade within two weeks of injury and at 1, 3, 6, and 12 months after injury. Of SCI patients classified as ASIA -A within 15 d of injury, 71.7% were still A at six months post-injury, 16.2% had ASIA-B, 4.7% had ASIA-C, 6.8% had ASIA-D, and 0.5% had converted to ASIA-E., And only 25% of patients initially analyzed using ASIA-B remained B, and most converted to C and D. More than 70% of ASIA-C converted to D, while nearly 90% of ASIA-D did not29). In recent years, it has been reported that the ASIA Impairement Scale conversion rate of patients with complete SCI has increased compared to the past30), which is thought to be due to the influence of the management of mean arterial blood pressure and the development of surgical techniques in managing traumatic SCI. In this study, the number of patients who had ASIA-A in the initial evaluation decreased from 15% to 1.9% at 6 months after injury, showing a significantly high ASIA Impairment Scale conversion rate.
Components of secondary SCI, such as neuropathy, microhemorrhage, ischemia-reperfusion injury, and apoptosis, are major targets for prophylactic intervention and treatment in patients with acute SCI31). Although methylprednisolone had been spotlighted as a treatment regimen to prevent this secondary SCI, In NASCIS II and III, which were adopted by organizations worldwide, there is no proven evidence that methylprednisolone makes neurological improvement8,32). In addition, some studies have pointed out that high-dose steroid use in patients with acute spinal cord injury is skeptical because of the risk of serious side effects compared to the neurological benefits8). On the other hand, some studies have still shown benefits from the use of high-dose methylprednisolone33). To date, there is no clear alternative to steroids to the preventive intervention of secondary SCI. Even the slight improvement in sphincter control or finger motor function reported in NASICS trials can have a decisive effect on a patient's life. Therefore, some argue that it may be ethically justified to use drugs with potential efficacy in patients with SCI20). In our department, high-dose steroid therapy is not used in elderly patients. This is because there is currently insufficient evidence to support the benefits of steroid use versus side effects. However, in a young, severe SCI patients, methylprednisolone 500-mg/day was started, and the dose was gradually reduced over seven days. Methylprednisolone-treated patients showed improvement in lower extremity muscle strength and ASIA grade 6 months after injury, and there was one serious side effect along with fever due to leukemoid reaction. However, caution is needed in the interpretation of the efficacy of methylprednisolone use in this retrospective study because the steroid treatment group was characterized by relatively young age and severe injuries.
Many spine surgeons have agreed on the benefits of early surgery in SCI patients with spinal cord compression or spinal instability. However, there is no consensus on the most favorable time for surgery, as it varies from study to study, such as within 36 hours or within 72 hours34-37). In a prospective cohort study of 313 patients with acute SCI, Fehlings et al. found that the group that underwent surgery at a mean of 14 hours showed at least a grade 2 improvement in the ASIA injury scale after 6 months compared to the group that underwent surgery at a mean of 48 hours35). And Haldrup et al suggested that patients who underwent surgery within 24 hours had better neurological outcomes 1 year after trauma than those who underwent surgery after 24 hours36). In this study, 30 patients (34.48%) who underwent surgery within 36 hours showed relatively greater improvement in lower extremity strength 3 weeks after injury. Early surgical treatment shortens the ICU hospital stay, reduces complications, and improves neurological outcomes, so we suggest that early surgery is recommended except for patients who are difficult to operate due to unstable vital signs.
The comorbidity of traumatic brain injury (TBI) is reported in 16%-59%38), and this comorbidity is an important problem that increases the probability of early death in patients with spinal cord injury by 370%39). In this study, 66 (64.7%) patients had a head impact and underwent an initial brain CT scan. Of these, nine (13.6%) patients with contusion, hemorrhage with or without skull fracture were observed using a CT scan. TBI's severity may interfere with the reliability of the initial neurological examination, which is vital as it may interfere with patient treatment planning and outcome prediction. High conversion rates can be shown in early hours or days after injury in patients with complete SCI who are misclassified due to inaccurate initial neurological examination40).
This study has some drawbacks because it was a retrospective study conducted at a single institution. There were limits to the control of various variables that could affect the prognosis, such as the extent and severity of SCI, the mechanism of trauma, and the underlying diseases. In addition, a bias is expected because steroid administration subjects were not randomly selected, but relatively young patients with few underlying diseases were selected. However, we tried to reduce the heterogeneity of patients by limiting the study subject to SCI patients who require treatment in the ICU. Short-term and long-term prognosis were analyzed with various risk factors. In addition, the prevalence of infection sites and microorganisms in SCI patients was thoroughly investigated. These data are expected to provide useful information for the treatment of SCI. And although caution is required in interpretation, the findings that steroid use and early surgery improved the prognosis of patients with spinal cord injury suggest that further studies on these treatments are still needed.
CONCLUSION
SCI causes different fatal complications, and treatment for these complications is critical in preventing secondary damage to the spinal cord and decreasing morbidity in patients. In this study, early surgery within 36 hours of injury was meaningful in improving lower extremity motor grade after 3 weeks in SCI patients, and it was observed that the ASIA injury scale was further improved at 6 months of injury in patients receiving high-dose steroids.