

INTRODUCTION
Initially described in 1921, Creutzfeldt-Jakob disease (CJD) is a rare, transmissible prion disease1). There are four types of CJD known. Sporadic, familial, iatrogenic and variant, of which sporadic Creutzfeldt-Jakob disease (sCJD) is the most common, and sCJD has characteristic clinical and diagnostic features2-4). It is a rapidly progressive, deadly infectious disease that usually results in death within a year of onset3,4).
The disease is thought to be caused by an abnormal isoform of a cellular glycoprotein known as prion protein, and is found in about 1 in 1 million people4-6). Sporadic Creutzfeldt-Jakob disease, like other prion diseases, is classified as a transmissible spongiform encephalopathy and occurs as a sporadic disease without a recognizable transmission pattern in approximately 85% of patients6). Current criteria for diagnosis include a distinct phenotype, periodic sharp and slow-wave complexes at electroencephalography (EEG), and a positive 14-3-3-protein assay in the cerebrospinal fluid (CSF). But the definitive diagnostic method for sCJD is neuropathologic or immunodiagnostic testing of brain tissue through biopsy or autopsy5-7).
Neuropsychiatric symptoms are relatively common in the early stage of variant Creutzfeldt-Jakob disease (vCJD), but psychiatric manifestations are reported to be rare in the clinical features of sCJD8,9).
In this case report, we would like to report a case in which a patient with unusual visual hallucination was diagnosed with CJD.
CASE REPORT
A 57-year-old female patient visited the emergency room with seizure, visual Hallucination, cognitive decline, left limb weakness, and gait disturbance that occurred 2 days before admission.
She had a history of being admitted to a psychiatric hospital for heavy alcohol use. The patient showed signs of recovery in consciousness and limb weakness during treatment in the intensive care unit for several days, but disorientation of places and people and hallucinations and illusions continued intermittently. In particular, she showed a continuous virtual conversation with family members who did not reside next to her, and When the medical staff asked about this, she mistakenly thought it was her son and continued talking. Sometimes, when the medical staff talked to her during the examination, she was excessively afraid, saying that she looked like a blank face when seeing the medical staff and she also was aggressive in accusing the medical staff of appearing too big a monster.
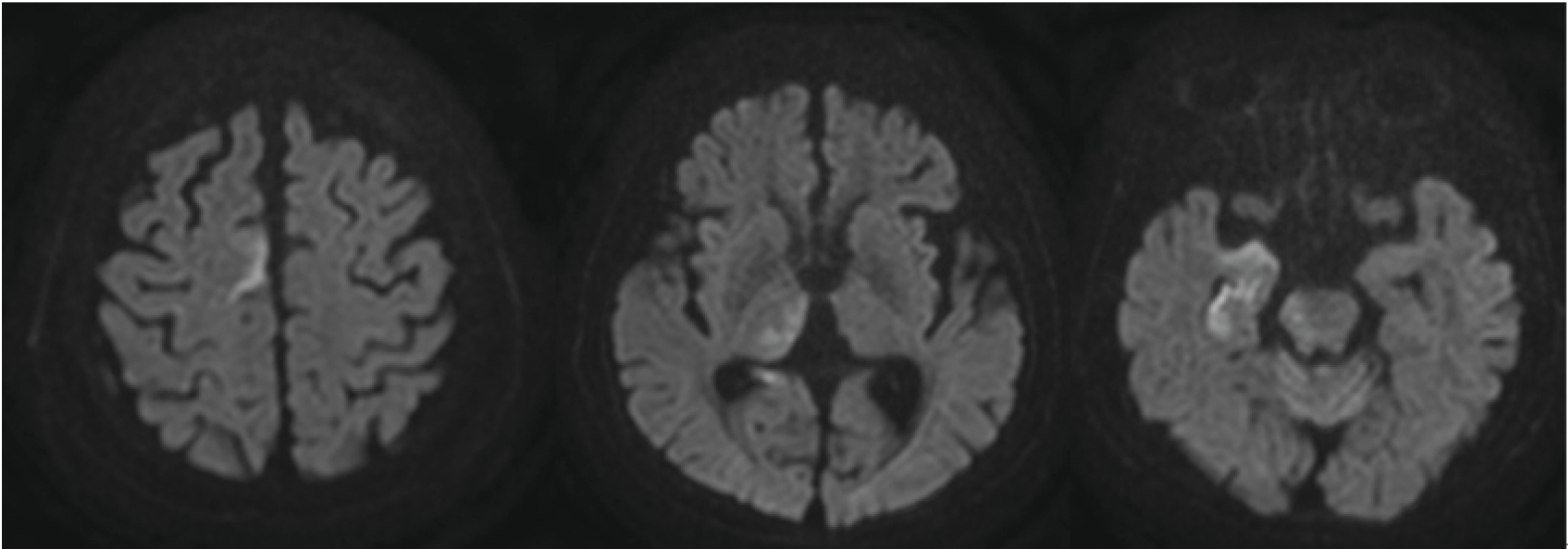
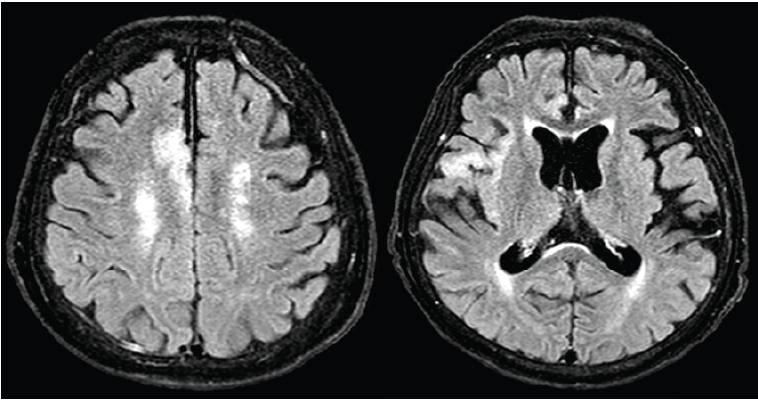
We performed brain magnetic resonance imaging (MRI) after admission, on the diffusion weighted and T2 FLAIR image, high signal intensity lesions were observed in the medial frontal cortex, right hippocampus, right insular cortex, right temporal cortex, and right thalamus including the right cingulate gyrus. (Figs. 1, 2) For further evaluation, cerebrospinal fluid (CSF) analysis was performed through lumbar, we checked positive findings of 14-3-3 protein test.
We were finally diagnosed with sCJD, and after about 2 weeks of treatment in the neurosurgery intensive care unit (NCU), the patient's symptoms improved. After fully explaining to the patient's family that there is no treatment for the disease and the poor prognosis, she was discharged on the 13th day of hostital day. We planned follow-up through outpatient treatment.
DISCUSSION
Various psychiatric symptoms such as sleep disturbance, psychosis, depressive, and behavioral dyscontrol anxiety are rarely reported in sCJD10,11). Among them, there was a case that reported visual hallucination as in this case12,13).
The mechanism by which these symptoms occur in sCJD is not known, but it is thought to be related to the limbic system. Limbic system damage was also observed in some cases we investigated, and in this case, limbic system damage is also suspected. In some cases, medication was needed, but in most cases it improved12-14).